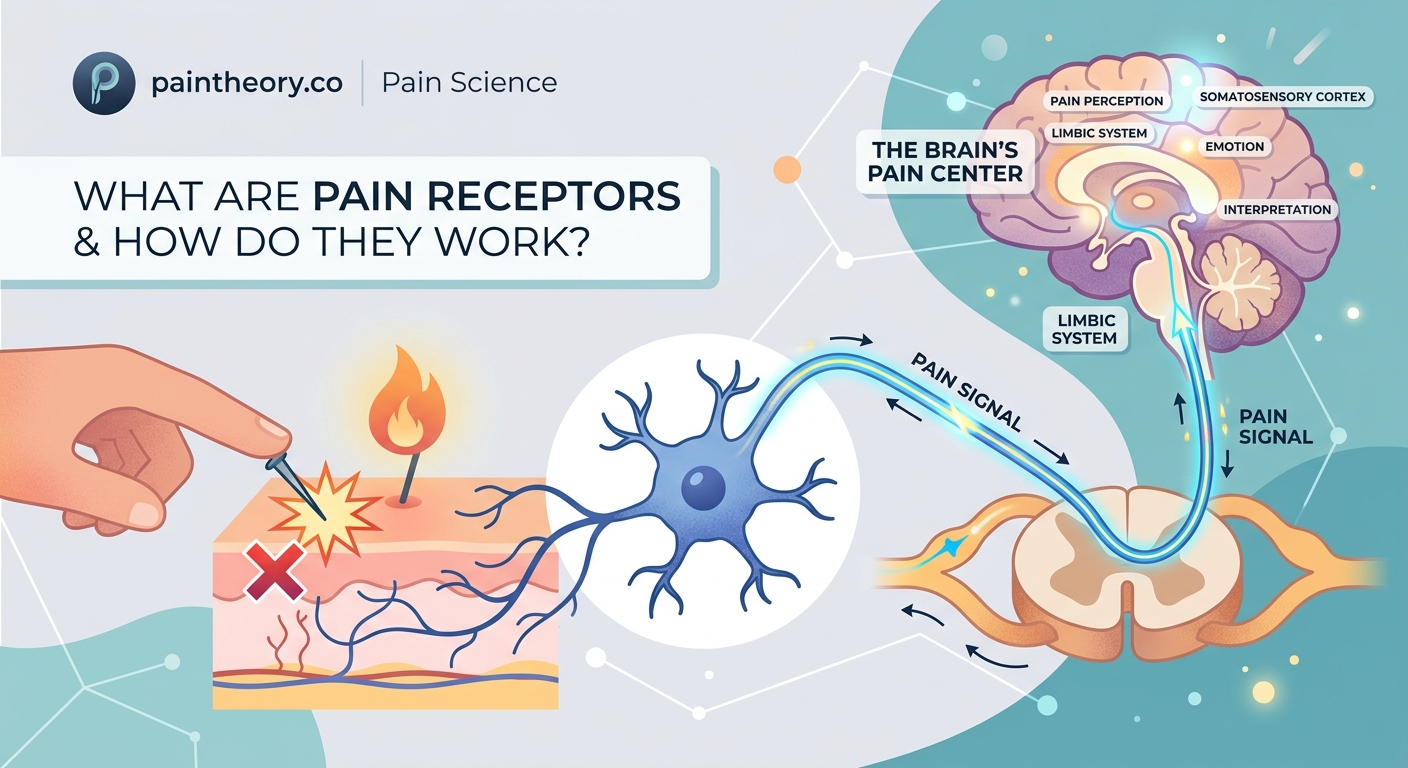
You touch a hot stove and yank your hand back before you even think about it. That split-second reaction happens because specialized nerve endings called pain receptors are already firing signals through your body. But what exactly triggers these receptors, and how does a physical sensation become the conscious experience of pain?
Pain receptors, called nociceptors, are specialized nerve endings that detect harmful stimuli like extreme heat, pressure, or chemical damage. When activated, they convert these threats into electrical signals that travel through nerve pathways to your spinal cord and brain, where the sensation is interpreted as pain. This system protects your body by alerting you to potential injury.
What Pain Receptors Actually Are
Pain receptors aren’t like the sensors in your smartphone. They’re free nerve endings scattered throughout your body, with the highest concentrations in your skin, joints, and internal organs.
Scientists call them nociceptors, from the Latin word “nocere,” meaning to harm. Unlike other sensory receptors that respond to light touch or temperature, nociceptors only activate when something threatens tissue damage.
Your body contains millions of these receptors. They sit at the tips of specialized nerve fibers, waiting to detect danger.
Three main types exist:
- Mechanical nociceptors respond to intense pressure, cuts, or crushing forces
- Thermal nociceptors detect extreme heat or cold
- Polymodal nociceptors react to multiple threats including chemicals released by damaged cells
That last type is the most common. When you stub your toe, polymodal nociceptors pick up both the impact and the inflammatory chemicals your injured tissue releases.
The Signal Journey From Tissue to Brain
Understanding how pain receptors work means following the signal from start to finish. This process happens in distinct stages, each taking only milliseconds.
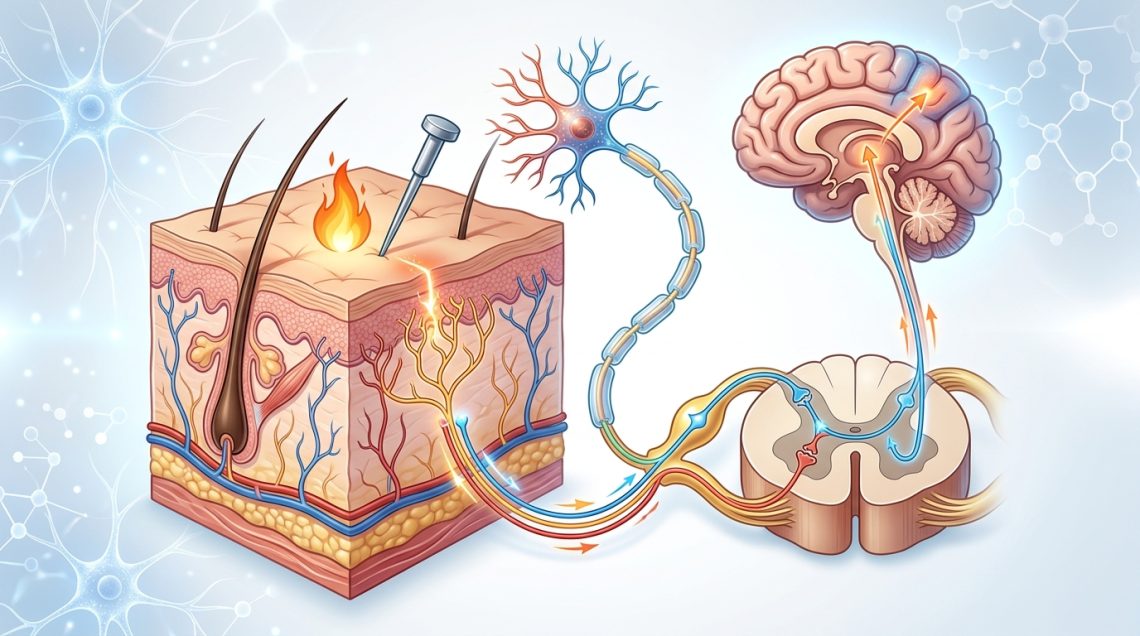
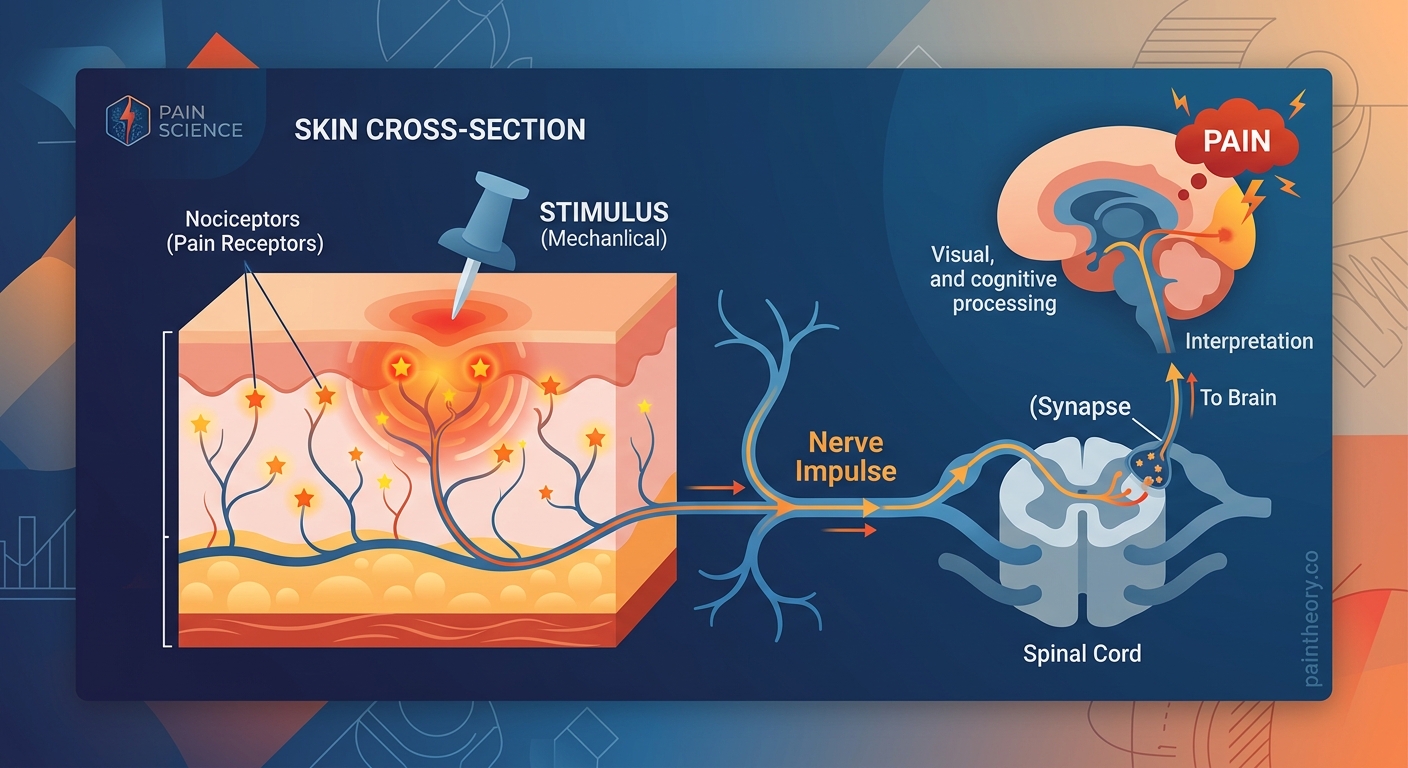
Stage 1: Detection and Activation
When tissue damage occurs, your cells release chemicals like bradykinin, prostaglandins, and substance P. These molecules bind to nociceptor endings and trigger them to fire.
The receptor converts this chemical or physical stimulus into an electrical signal called an action potential. Think of it like flipping a switch that starts a chain reaction.
Temperature extremes work differently. Thermal nociceptors contain special proteins that change shape when exposed to heat above 109°F or cold below 59°F. This shape change opens ion channels, letting charged particles rush into the nerve ending and generating the electrical signal.
Stage 2: Transmission Through Nerve Fibers
Once activated, the signal travels along nerve fibers toward your spinal cord. Two types of fibers carry pain signals:
A-delta fibers are thinly insulated and transmit signals at about 40 miles per hour. These create the sharp, immediate pain you feel when you cut your finger.
C fibers lack insulation and move signals at roughly 2 miles per hour. They produce the dull, throbbing ache that follows the initial sharp pain.
This two-speed system explains why pain often comes in waves. The fast signal hits first, then the slower, deeper pain arrives seconds later.
Stage 3: Processing in the Spinal Cord
Your spinal cord isn’t just a highway for signals. It’s a processing center that can amplify, reduce, or even block pain messages before they reach your brain.
Nerve fibers entering the spinal cord connect with interneurons in an area called the dorsal horn. These interneurons decide which signals get forwarded to the brain and which get dampened.
This is where the famous “gate control theory” operates. Non-painful input like rubbing an injury can close the gate by activating other nerve fibers that inhibit pain transmission. That’s why massaging a sore muscle actually helps.
Stage 4: Brain Interpretation
Pain signals that make it past the spinal cord travel to multiple brain regions:
- The thalamus acts as a relay station, directing signals to other areas
- The somatosensory cortex identifies where the pain is located and how intense it feels
- The limbic system adds emotional context, making pain feel unpleasant or distressing
- The prefrontal cortex evaluates the meaning and decides how to respond
Your brain doesn’t just passively receive pain signals. It actively constructs the pain experience based on context, past experiences, and current emotional state. The same injury can feel more or less painful depending on these factors, which explains why your brain creates and amplifies pain sensations in ways that seem disconnected from tissue damage.
Why Different Injuries Feel Different
The quality of pain you experience depends on which receptors activate and how your nervous system processes their signals.
| Pain Type | Receptor Involved | Fiber Type | Characteristics |
|---|---|---|---|
| Sharp, stabbing | Mechanical nociceptors | A-delta | Immediate, well-localized, brief |
| Burning | Thermal nociceptors | A-delta and C | Intense, spreads slightly, persistent |
| Aching, throbbing | Polymodal nociceptors | C | Delayed onset, poorly localized, long-lasting |
| Cramping | Visceral nociceptors | C | Deep, diffuse, often nauseating |
Visceral pain from internal organs feels different because these organs have fewer nociceptors spread over larger areas. You can’t pinpoint exactly where your stomach hurts the way you can locate a paper cut.
The brain also interprets visceral pain signals less precisely, sometimes projecting them to skin areas that share nerve pathways. This is called referred pain. Heart attack pain radiating to the left arm happens because heart nerves and arm nerves converge at the same spinal cord level.
When Pain Signals Go Wrong
Sometimes the pain system malfunctions, creating sensations without actual tissue damage. This happens when nerves become oversensitive or the nervous system fails to properly regulate pain signals.
“Chronic pain often represents a nervous system that has learned to be too good at its job. The alarm keeps ringing even after the danger has passed.” — Pain neuroscience researchers
Sensitization occurs when repeated activation makes nociceptors fire more easily. Inflammatory chemicals lower their threshold, so even gentle touch can trigger pain signals. This is why sunburned skin hurts when you brush against it.
Central sensitization happens when spinal cord and brain neurons become hyperexcitable. They amplify normal signals and generate pain from non-painful input. Understanding why pain becomes chronic requires recognizing these changes in how your nervous system processes signals.
Nerve damage creates a different problem. Injured nerve fibers can fire spontaneously or develop abnormal sensitivity to mechanical pressure or chemical signals. This produces neuropathic pain that feels like burning, shooting, or electric shocks.
The Body’s Built-In Pain Control
Your nervous system contains natural pain relief mechanisms that work alongside pain receptors.
Descending pathways from the brain can suppress pain signals in the spinal cord. When you’re focused on something important or in a high-stress situation, these pathways release neurotransmitters like serotonin and norepinephrine that reduce pain transmission.
This explains why athletes sometimes don’t notice injuries during competition or why soldiers report feeling less pain in combat situations.
Your body also produces endogenous opioids, natural chemicals similar to morphine. These bind to receptors on nociceptors and spinal cord neurons, blocking pain signal transmission. Exercise, laughter, and even certain foods can trigger endorphin release.
The placebo effect demonstrates how powerfully your brain can modulate pain. When you believe a treatment will help, your brain activates these descending pain control systems, producing real pain relief even from inactive substances.
Common Misconceptions About Pain Receptors
Misconception: More tissue damage always means more pain.
Reality: Pain intensity doesn’t directly correlate with injury severity. Small nerve injuries can cause excruciating pain while major internal damage sometimes produces minimal discomfort initially.
Misconception: Pain receptors only exist in injured tissue.
Reality: Nociceptors are present throughout healthy tissue, constantly monitoring for threats. They only send signals when activated by potentially harmful stimuli.
Misconception: Blocking pain receptors eliminates all pain.
Reality: Pain involves multiple pathways and brain regions. Local anesthetics block peripheral signals, but central nervous system processing continues. This is why some pain persists even after nerve blocks.
Misconception: Pain tolerance is fixed.
Reality: Your pain experience changes based on context, expectations, stress levels, and previous experiences. The same receptor activation can feel more or less painful depending on these factors.
Factors That Influence Pain Receptor Sensitivity
Several conditions alter how responsive your nociceptors are:
Inflammation releases chemicals that lower activation thresholds. Prostaglandins, bradykinin, and nerve growth factor make receptors fire more easily and more frequently.
Temperature affects nerve conduction speed. Cold initially numbs pain by slowing signal transmission, while heat can increase sensitivity by speeding up chemical reactions in nerve tissue.
Hormones modulate pain perception throughout your menstrual cycle. Estrogen influences nociceptor sensitivity and central pain processing, which partly explains how hormones amplify chronic pain in certain conditions.
Sleep deprivation increases pain sensitivity by disrupting descending pain control systems and lowering pain thresholds in the brain.
Stress has complex effects. Acute stress can reduce pain through adrenaline and endorphin release, while chronic stress sensitizes pain pathways and increases inflammatory signaling.
How Medical Treatments Target Pain Receptors
Understanding pain receptor function has led to targeted treatments:
NSAIDs like ibuprofen block enzymes that produce prostaglandins, reducing nociceptor sensitization at the injury site.
Local anesthetics prevent action potential generation by blocking sodium channels in nerve membranes. Signals can’t travel if the electrical impulse can’t form.
Capsaicin cream initially activates then depletes substance P from nerve endings, temporarily reducing their ability to transmit pain signals.
Nerve blocks use anesthetics or steroids near specific nerves to interrupt signal transmission. This works well for localized pain from identifiable sources.
Opioid medications bind to receptors in the spinal cord and brain, mimicking your body’s natural pain control chemicals. Comparing pain medications helps you understand which approach works best for different pain types.
Physical interventions also affect pain receptors. Heat increases blood flow and reduces muscle tension, while cold decreases inflammation and slows nerve conduction.
The Protective Purpose of Pain
Pain receptors exist to protect you. Without them, you’d unknowingly damage your body through burns, cuts, broken bones, and internal injuries.
People born with congenital insensitivity to pain lack functional nociceptors. They suffer repeated injuries, infections, and joint damage because they can’t detect tissue damage. Most don’t survive past their twenties.
Pain teaches you to avoid harmful situations. The memory of touching a hot stove makes you more careful around heat sources. This learning happens both consciously and through automatic reflexes.
Withdrawal reflexes bypass your brain entirely. When you step on something sharp, spinal cord circuits trigger leg muscles to pull away before the pain signal reaches conscious awareness. This reflex arc can save tissue from further damage.
Internal pain signals problems you can’t see. Appendicitis pain prompts medical care before rupture occurs. Chest pain during a heart attack alerts you to seek emergency treatment.
The challenge comes when pain persists after healing or when the system becomes oversensitive. Recognizing back pain red flags helps distinguish protective pain from dysfunction that needs medical evaluation.
What This Means for Managing Your Pain
Knowing how pain receptors work changes how you approach pain management.
First, inflammation control matters. Reducing the chemicals that sensitize nociceptors can break the cycle of increasing pain sensitivity.
Second, timing affects treatment success. Addressing pain early prevents central sensitization from developing. Chronic pain becomes harder to treat once nervous system changes occur.
Third, multiple approaches work better than single interventions. Combining physical treatments that affect peripheral receptors with strategies that target central processing produces better results than either alone.
Fourth, context influences your pain experience. Managing stress, improving sleep, and maintaining social connections all affect how your nervous system processes pain signals.
Finally, understanding that pain doesn’t always equal damage helps you make better decisions. Sometimes movement helps even when it initially hurts, while other times rest is essential. Learning to interpret your body’s signals takes practice.
Your pain receptors are sophisticated sensors doing exactly what evolution designed them to do. They detect threats, send warnings, and protect your body from harm. When they work properly, they’re invaluable. When they malfunction, understanding their biology helps you find effective solutions.