You stub your toe, feel the sharp sting, and within days the pain fades. That’s how pain is supposed to work. But for millions of people, pain doesn’t follow this script. It lingers for months or years, long after tissues heal. The injury becomes a memory, but the pain stays vivid and real.
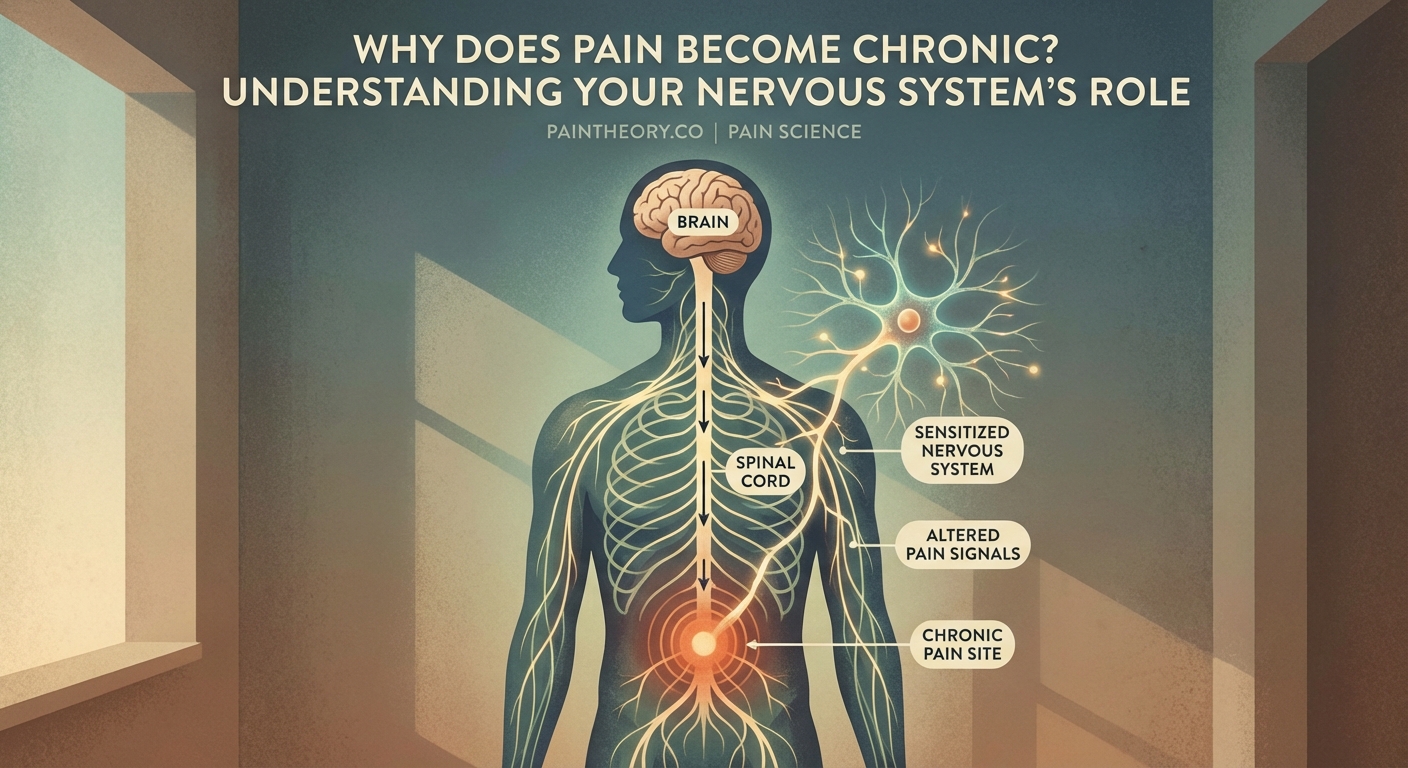
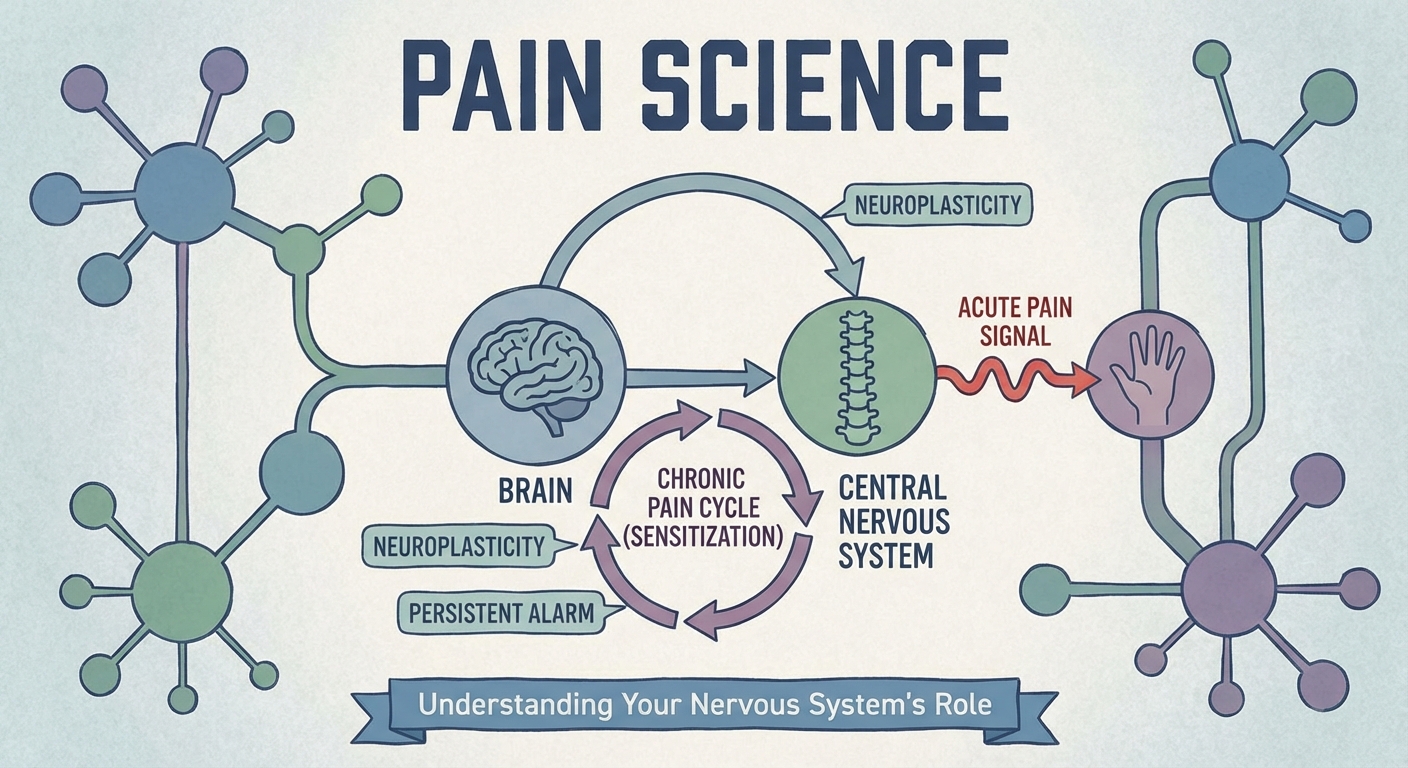
Pain becomes chronic when your nervous system changes how it processes signals. Through central sensitization, neural rewiring, and amplified responses, your body maintains pain even after healing. These biological shifts involve your spinal cord, brain structures, and neurotransmitter systems, creating a persistent pain state that requires understanding these mechanisms to address effectively.
How Normal Pain Processing Works
Your body designed pain as a warning system. Touch a hot stove and specialized nerve endings called nociceptors detect tissue damage. They send electrical signals up your spinal cord to your brain. Your brain interprets these signals, creates the sensation you recognize as pain, and triggers protective responses.
This system works beautifully for acute injuries. The pain intensity matches the damage level. As tissues heal, inflammation decreases, and pain signals fade. Within weeks or months, the alarm turns off.
But sometimes this system malfunctions.
The nervous system can change its own wiring. It can amplify signals, lower thresholds, and maintain alert status long after danger passes. These changes transform acute pain into a chronic condition that persists for three months, six months, or decades.
The Transition From Protective Signal to Persistent Problem
Pain becomes chronic through a series of biological changes that happen at multiple levels of your nervous system. These aren’t imaginary or psychological. They’re measurable physical alterations in how your nerves, spinal cord, and brain function.
Three Pathways That Lead to Chronicity
-
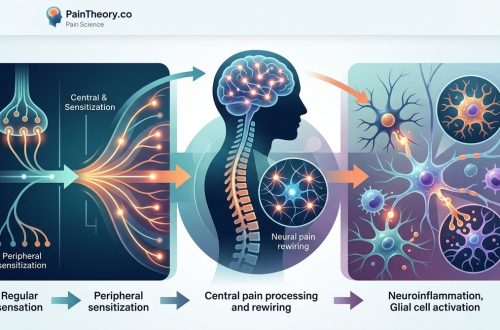
Peripheral sensitization: Damaged nerves or ongoing inflammation makes nerve endings more sensitive. They fire more easily and send stronger signals. A light touch that shouldn’t hurt starts triggering pain responses.
-
Central sensitization: Your spinal cord and brain increase their responsiveness to incoming signals. They turn up the volume on pain messages. Normal sensations get interpreted as threats.
-
Structural brain changes: Prolonged pain alters brain anatomy. Gray matter volume changes in pain processing regions. Neural connections reorganize. Your brain literally rewires itself around the experience of pain.
Each pathway can operate independently, but they often work together, creating a self-reinforcing cycle that makes pain increasingly difficult to resolve.
Central Sensitization Amplifies Everything
Central sensitization represents one of the most important concepts for understanding why pain persists. Your spinal cord acts as a relay station between your body and brain. Normally, it passes along pain signals without much modification.
But repeated or intense pain signals change how this relay station operates. Nerve cells in your spinal cord become more excitable. They respond to weaker stimuli. They recruit neighboring neurons that normally handle other sensations like touch or pressure.
This creates several noticeable effects:
- Pain spreads beyond the original injury site
- Light touch or gentle pressure causes pain (allodynia)
- Painful stimuli hurt more than they should (hyperalgesia)
- Pain persists even when triggers are removed
- Multiple body areas become sensitive simultaneously
Your nervous system essentially gets stuck in a heightened state of alert. It interprets normal sensory input as dangerous, maintaining pain long after any real threat has passed.
Brain Structures That Change With Chronic Pain
Research using brain imaging has revealed specific structural and functional changes in people with chronic pain. These aren’t subtle. They’re significant enough to see on MRI scans.
The prefrontal cortex, which handles decision making and emotional regulation, shows decreased gray matter volume in chronic pain patients. The anterior cingulate cortex, involved in pain perception and emotional processing, becomes hyperactive.
The amygdala, your brain’s threat detection center, grows more reactive. It amplifies emotional responses to pain and increases anxiety about future pain. This creates a feedback loop where fear of pain actually intensifies pain sensations.
The hippocampus, critical for memory and learning, often shows reduced volume. This may explain why chronic pain affects memory and concentration. Your brain devotes so many resources to processing pain that other cognitive functions suffer.
These changes aren’t permanent or irreversible. The same neuroplasticity that allows pain to become chronic also offers hope for recovery. Brains can rewire themselves in healthier directions with appropriate treatment.
The Role of Neurotransmitters and Chemical Messengers
Your nervous system relies on chemical messengers called neurotransmitters to transmit signals between nerve cells. Chronic pain disrupts the normal balance of these chemicals.
Glutamate, the primary excitatory neurotransmitter, increases in chronic pain states. More glutamate means more nerve activation and stronger pain signals. Meanwhile, GABA, the main inhibitory neurotransmitter that dampens nerve activity, often decreases. This combination removes the brakes while pressing the accelerator.
Substance P, a neuropeptide involved in pain transmission, accumulates in the spinal cord. Higher levels of substance P make nerve cells more sensitive and responsive to pain signals.
Serotonin and norepinephrine, which normally help modulate pain, become dysregulated. These neurotransmitters usually activate descending pathways that reduce pain signals. When their systems malfunction, you lose this natural pain control mechanism.
| Neurotransmitter | Normal Function | Change in Chronic Pain | Effect on Pain |
|---|---|---|---|
| Glutamate | Excites nerve cells | Increases | Amplifies pain signals |
| GABA | Inhibits nerve activity | Decreases | Reduces pain control |
| Substance P | Transmits pain signals | Accumulates | Heightens sensitivity |
| Serotonin | Modulates pain perception | Dysregulated | Weakens pain inhibition |
| Norepinephrine | Reduces pain signals | Dysregulated | Impairs natural pain relief |
Why Some People Develop Chronic Pain and Others Don’t
Not everyone who experiences acute pain develops chronic pain. Certain risk factors increase vulnerability to this transition.
Genetic factors play a role. Some people inherit variations in genes that control pain signaling, inflammation, or stress responses. These genetic differences don’t guarantee chronic pain, but they influence susceptibility.
Previous pain experiences matter. Someone who has already had one episode of chronic pain faces higher risk for developing it again. The nervous system retains a kind of memory of past pain states.
Psychological factors influence outcomes. High levels of stress, anxiety, depression, or catastrophic thinking about pain correlate with increased risk of chronicity. These aren’t the cause of pain, but they affect how the nervous system processes and responds to pain signals.
The initial injury severity doesn’t always predict who develops chronic pain. Some people with minor injuries develop severe chronic pain, while others with major trauma recover completely. This paradox highlights how chronic pain depends more on nervous system changes than ongoing tissue damage.
“Chronic pain is not simply prolonged acute pain. It represents a fundamental shift in how the nervous system functions. The pain itself becomes the disease, rather than a symptom of injury.”
Common Conditions Where Acute Pain Turns Chronic
Certain injuries and conditions more frequently lead to chronic pain. Understanding these patterns helps explain why pain persists.
Back injuries represent one of the most common sources of chronic pain. An initial muscle strain or disc injury can trigger changes in spinal cord processing that outlast the tissue healing. The nervous system maintains protective muscle tension and pain signals even after structural healing completes.
Nerve injuries carry particularly high risk. When nerves themselves get damaged, they can develop abnormal firing patterns. They send pain signals spontaneously, without any external trigger. This neuropathic pain often feels like burning, shooting, or electric sensations.
Complex regional pain syndrome (CRPS) demonstrates how dramatically the nervous system can malfunction. A minor injury like a sprained ankle triggers an exaggerated inflammatory response and nervous system changes that cause severe, spreading pain far out of proportion to the original injury.
Post-surgical pain becomes chronic in 10 to 50 percent of patients, depending on the surgery type. Procedures that involve cutting nerves or extensive tissue trauma carry higher risk. The surgical healing process itself can trigger central sensitization.
The Inflammatory Connection
Inflammation plays a complex role in the transition from acute to chronic pain. Normal inflammation helps healing. It brings immune cells and growth factors to damaged tissues. This inflammatory response should resolve as healing progresses.
But sometimes inflammation persists at low levels even after tissues heal. This chronic low-grade inflammation keeps nociceptors activated and sensitive. It maintains a constant stream of pain signals to the spinal cord and brain.
Inflammatory molecules called cytokines can directly sensitize nerve cells. They lower the threshold for nerve activation and increase the strength of pain signals. Some cytokines even promote structural changes in the nervous system that maintain chronic pain.
Certain conditions involve systemic inflammation that affects the entire body. Autoimmune diseases, metabolic syndrome, and chronic infections create an inflammatory environment that increases pain sensitivity throughout the nervous system.
Emotional and Cognitive Factors That Maintain Pain
Your brain doesn’t process pain signals in isolation. It integrates them with emotions, memories, attention, and beliefs. This integration means psychological factors significantly influence whether pain becomes chronic.
Fear of pain creates a self-fulfilling prophecy. When you expect movement to hurt, your nervous system primes itself for pain. Muscle tension increases. Attention focuses on body sensations. The brain interprets ambiguous signals as threatening. This hypervigilance amplifies pain perception.
Stress hormones like cortisol affect pain processing. Acute stress can temporarily reduce pain through the fight-or-flight response. But chronic stress sensitizes the nervous system and increases pain over time.
Depression and chronic pain share overlapping brain circuits. The same neurotransmitter systems that regulate mood also modulate pain. This explains why depression increases pain sensitivity, and why chronic pain frequently leads to depression.
Attention acts like a spotlight. Where you focus your attention determines what your brain processes most intensely. Constantly monitoring pain sensations strengthens the neural pathways involved in pain perception. Your brain dedicates more processing power to pain, making it more prominent in your conscious experience.
The Descending Pain Modulation System
Your brain doesn’t just passively receive pain signals. It actively controls how much pain you feel through descending pathways that travel from the brain back down to the spinal cord.
These pathways can either increase or decrease pain signals before they reach conscious awareness. When functioning properly, they provide natural pain relief. The periaqueductal gray and rostral ventromedial medulla, brain regions involved in this system, release neurotransmitters that inhibit pain transmission.
This system explains phenomena like soldiers who don’t notice serious injuries during combat, or athletes who play through pain during competition. Strong descending inhibition can temporarily block pain signals when other priorities take precedence.
But chronic pain impairs this natural pain control system. The descending pathways become less effective at inhibiting pain. Some pathways may even switch from inhibitory to facilitatory, actually increasing pain signals rather than reducing them.
Restoring proper function to descending pain modulation represents an important target for chronic pain treatment. Techniques that activate these pathways can help reduce pain intensity.
Memory and Learning in Chronic Pain
Your nervous system learns from experience. Repeated pain signals teach your brain to expect and respond to pain more readily. This pain memory contributes to chronicity.
Neurons that fire together wire together. When pain signals repeatedly activate certain neural pathways, those connections strengthen. The pathway becomes more efficient, requiring less input to produce the same pain response. Eventually, the pathway may activate spontaneously, creating pain without any external trigger.
The brain also forms associations between pain and specific contexts, movements, or situations. If bending forward repeatedly caused pain, your brain may start generating pain signals in anticipation of bending, even before any actual tissue stress occurs.
This learned pain response isn’t conscious or voluntary. It happens at a neural level below awareness. You can’t simply decide to stop these automatic responses. But understanding their existence helps explain why chronic pain persists and why treatment must address these learned patterns.
When Pain Spreads Beyond the Original Site
One puzzling feature of chronic pain is how it often spreads to areas far from the initial injury. Someone with a knee injury develops hip and back pain. A shoulder injury leads to neck pain and headaches.
This spreading occurs because of changes in central pain processing. As the spinal cord becomes sensitized, it starts interpreting signals from neighboring body regions as painful. The brain’s body map, which normally maintains clear boundaries between different areas, becomes blurred.
Referred pain patterns contribute to spreading. The spinal cord segments that receive signals from one body part also receive input from other areas. When central sensitization occurs, the nervous system can’t distinguish between these different sources, causing pain to spread.
Protective movement patterns also play a role. When one area hurts, you unconsciously alter how you move to avoid pain. These compensatory movement patterns create stress on other body parts, potentially triggering pain in those regions too.
The Timeline of Nervous System Changes
The transformation from acute to chronic pain doesn’t happen overnight. It unfolds over weeks and months through a predictable sequence of changes.
Days to weeks: Peripheral sensitization develops at the injury site. Inflammatory molecules accumulate. Nerve endings become more sensitive. Pain intensity may actually increase during this period even as tissues begin healing.
Weeks to months: Central sensitization emerges in the spinal cord. Nerve cells become more excitable. The area of sensitivity expands. Pain starts responding less predictably to typical triggers.
Months to years: Brain structure and function change. Gray matter volume shifts. Neural connections reorganize. Descending pain control systems malfunction. Pain becomes increasingly disconnected from any ongoing tissue damage.
This timeline varies between individuals and depends on many factors including injury severity, treatment received, and individual vulnerability. But understanding this progression helps explain why early intervention matters so much for preventing chronic pain.
Measuring Nervous System Changes
Researchers can now measure many of the nervous system changes associated with chronic pain. These measurements help validate that chronic pain involves real, physical alterations in neural function.
Quantitative sensory testing assesses how the nervous system responds to various stimuli. It can detect increased sensitivity to pressure, temperature, or other sensations that indicate central sensitization.
Brain imaging techniques like functional MRI show which brain regions activate during pain. They reveal hyperactivity in pain processing areas and reduced activity in pain control regions.
Electroencephalography (EEG) measures electrical activity in the brain. It can detect abnormal patterns associated with chronic pain states.
Biomarkers in blood or cerebrospinal fluid reflect inflammatory processes and neurotransmitter changes. While not yet used routinely in clinical practice, these measurements help researchers understand pain mechanisms.
These objective measures confirm that chronic pain isn’t “all in your head” in the dismissive sense. It involves measurable biological changes in nervous system structure and function.
Breaking the Cycle
Understanding why pain becomes chronic points toward how to address it. Treatment must target the nervous system changes that maintain pain, not just the original injury.
Medications that modulate neurotransmitter systems can help restore chemical balance. Drugs that enhance GABA or reduce glutamate activity may decrease central sensitization.
Physical approaches that provide novel, non-painful sensory input can help retrain pain processing. Gentle movement, specific exercises, and manual therapy offer the nervous system new information that contradicts learned pain patterns.
Psychological techniques address the emotional and cognitive factors that maintain pain. Cognitive behavioral therapy helps modify pain-related thoughts and behaviors. Mindfulness meditation can reduce the emotional amplification of pain signals.
Neuromodulation techniques directly alter nervous system activity. Transcutaneous electrical nerve stimulation, spinal cord stimulation, or other approaches can activate descending pain control pathways or interrupt pain signal transmission.
The most effective approach typically combines multiple strategies that address different aspects of nervous system dysfunction. No single treatment reverses all the changes that maintain chronic pain.
Your Nervous System Can Change Again
The same neuroplasticity that allows pain to become chronic also enables recovery. Your nervous system retains the ability to reorganize itself throughout life.
Brains of people who recover from chronic pain show measurable changes. Gray matter volume normalizes. Hyperactive pain regions quiet down. Descending pain control systems regain function.
This recovery doesn’t happen automatically or instantly. It requires consistent input that teaches the nervous system to process signals differently. But the potential for change always exists.
Understanding the biological basis of chronic pain removes blame and shame. You didn’t cause these nervous system changes through weakness or poor coping. They represent your nervous system’s attempt to protect you, even when that protection becomes counterproductive.
This knowledge also provides direction. Treatment that addresses nervous system changes, rather than searching for ongoing tissue damage, offers the best chance for meaningful improvement.
Making Sense of Your Pain Experience
The science behind chronic pain helps explain experiences that might otherwise seem confusing or frightening. Pain that spreads, intensifies, or persists despite healing makes sense when you understand central sensitization and brain changes.
Knowing that your nervous system has physically changed validates your experience. The pain is real, even if scans show healed tissues. The problem lies in how your nervous system processes signals, not in your character or pain tolerance.
This understanding also suggests patience. Nervous system changes that developed over months or years won’t reverse in days or weeks. Recovery requires time for neural pathways to reorganize and for brain structures to normalize.
But recovery remains possible. Countless people have retrained their nervous systems and significantly reduced or eliminated chronic pain. Your biology isn’t your destiny. With appropriate treatment and consistent effort, the same plasticity that created chronic pain can support healing.