The first time you realize your body is hurting for no obvious reason, it feels like a betrayal. You didn’t twist the wrong way. You didn’t strain a muscle. You just woke up, or sat down, or leaned back, and there it was. A familiar ache. A burning tingle. A deep throb that has no business being there.
Here is the hard truth that most people miss. Pain is not a direct measure of tissue damage. It is a constructed experience. Your brain takes signals from your body, filters them through memory, emotion, and context, and then decides whether to let you feel pain. When that system works correctly, pain protects you. When it breaks down, normal sensations like a light touch or a gentle stretch get mislabeled as threats. This is not a psychological weakness. It is a physiological transformation. And it happens through three specific chronic pain mechanisms that researchers have now mapped in detail.
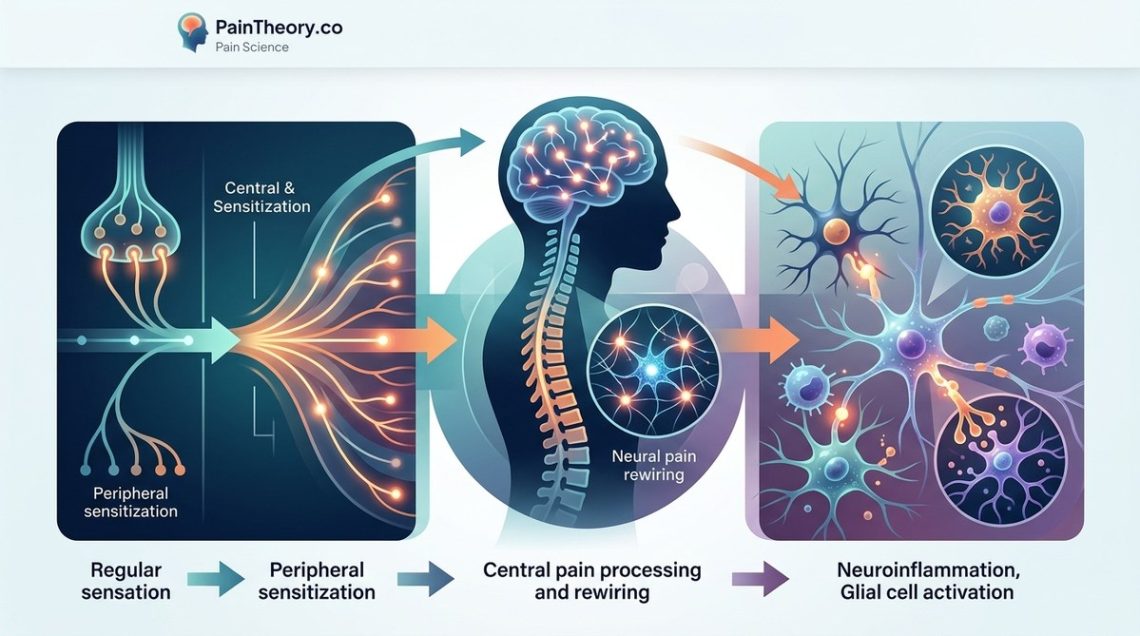
Chronic pain is not simply pain that lasts longer than expected. It is a distinct biological state driven by three mechanisms: peripheral sensitization, central sensitization, and impaired descending modulation. Each mechanism rewires how your nervous system processes sensation. Understanding these pathways helps you choose treatments that target the real problem, not just the symptom. Lasting relief starts with knowing what is actually broken.
What Actually Changes When Pain Becomes Chronic?
Acute pain is a warning system. You touch a hot stove, your hand pulls back, and the pain fades as the tissue heals. That is normal. Chronic pain is a malfunction of that warning system. The alarm keeps ringing even after the fire is out.
The shift from acute to chronic pain involves structural and functional changes in your nervous system. Your neurons actually change shape. They become more excitable. The connections between them strengthen in ways that make pain signals easier to send and harder to stop. These changes do not happen overnight. They build slowly, which is why early intervention matters so much.
Here is what researchers now know. The transition to chronic pain involves three distinct chronic pain mechanisms that work together like a feedback loop. Once this loop locks in, your body treats normal sensations as threats. A gentle pressure feels like a bruise. A warm shower feels like a burn. Movement itself becomes something to fear.
The Three Chronic Pain Mechanisms You Need to Know
Let me walk through each mechanism clearly. These are not abstract concepts. They are measurable biological processes that explain why your pain persists.
1. Peripheral Sensitization
Peripheral sensitization happens at the site of the original injury or irritation. Your nociceptors, which are the specialized nerve endings that detect harmful stimuli, become hypersensitive. They lower their firing threshold. A stimulus that would normally be harmless now triggers a pain signal.
Think of it like a smoke alarm that has been set to go off from steam instead of smoke. The alarm is not broken in the traditional sense. It is just way too sensitive. In the body, this happens because inflammatory chemicals like prostaglandins, substance P, and bradykinin accumulate around the nerve endings. These chemicals make the nerve membranes more permeable to sodium and calcium ions. That means the nerve fires more easily and more often.
Peripheral sensitization explains why your knee still hurts weeks after a minor twist. The original tissue might have healed, but the nerve endings in that area have not returned to their normal sensitivity. They are stuck in a state of high alert.
2. Central Sensitization
Central sensitization is the bigger player in chronic pain. This mechanism lives in your spinal cord and brain. It describes a state where the central nervous system itself becomes hyperexcitable. The volume knob for pain gets turned up and then locked in place.
Here is how it works. When pain signals arrive at the spinal cord repeatedly, they trigger a process called long term potentiation. The synapses between pain transmitting neurons become stronger. The neurons start releasing more glutamate, which is the main excitatory neurotransmitter in the brain. Receptors called NMDA receptors become more active. This combination makes it so that even a weak signal from the body gets amplified into a strong pain experience.
The really unsettling part is that central sensitization can spread. You might develop pain in areas far from the original injury. This is why someone with a low back injury can eventually feel pain in their hip, their leg, and even the opposite side of their body. The nervous system has generalized the threat response.
3. Impaired Descending Modulation
Your brain has natural painkillers. Serotonin, norepinephrine, and endogenous opioids all help tamp down incoming pain signals. These chemicals travel down from the brainstem to the spinal cord and block or reduce pain transmission. This is called descending inhibition.
In chronic pain, this descending inhibition system often stops working properly. The brain either stops releasing enough of these chemicals, or the spinal cord stops responding to them. On top of that, a separate system called descending facilitation can actually kick in and make pain worse. Your brain starts actively amplifying pain instead of quieting it.
This mechanism explains why many people with chronic pain do not get relief from standard painkillers. The problem is not just at the site of pain. It is in how the brain and spinal cord handle the signal. Medications that boost serotonin and norepinephrine, like certain antidepressants, can help restore descending inhibition. So can techniques like graded exercise and cognitive behavioral therapy, which retrain the brain’s pain processing pathways.
How These Chronic Pain Mechanisms Show Up in Daily Life
You might recognize these mechanisms without knowing their names. Here are some common experiences that map directly to each mechanism.
- Peripheral sensitization: Your lower back hurts when you lightly press on the skin over the muscle. Even clothing touching the area feels irritating.
- Central sensitization: Your pain spreads to your hip and thigh even though the original back injury was localized. Light activities like walking the dog now cause a flare up that lasts for hours.
- Impaired descending modulation: You feel pain even when resting in a comfortable position. Nothing you do seems to calm the sensation. Your nervous system appears to be running on its own.
These patterns are not random. They reflect which chronic pain mechanisms are driving your condition. Identifying the dominant mechanism helps you and your healthcare provider choose more targeted treatments.
Let me put this into a clearer framework.
| Mechanism | Where It Happens | What It Does | Best Treatment Approach |
|---|---|---|---|
| Peripheral sensitization | At the nerve endings in tissues | Lowers the threshold for nerve firing | Local anti inflammatories, nerve blocks, topical agents |
| Central sensitization | Spinal cord and brain | Amplifies all incoming pain signals | NMDA receptor antagonists, graded exposure therapy, pain neuroscience education |
| Impaired descending modulation | Brainstem and spinal pathways | Reduces natural pain inhibition | Serotonin norepinephrine reuptake inhibitors, aerobic exercise, cognitive behavioral therapy |
Why Most Treatments Fail When They Ignore These Mechanisms
A lot of people with chronic pain get stuck in a cycle of treatments that do not work. They try ice and heat. They stretch. They take over the counter pain relievers. None of it helps for long.
The reason is straightforward. If your chronic pain is driven by central sensitization, rubbing a muscle or icing a joint will not fix the problem. The issue is not in the tissue. It is in the spinal cord and brain. You cannot stretch your way out of a sensitized central nervous system any more than you can stretch your way out of a fever.
“The most important shift in pain science over the last twenty years is the recognition that chronic pain is a disease of the nervous system, not a persistent injury. Treating the tissue when the problem is neural is like repairing the windows when the thermostat is broken.” Dr. Adriaan Louw, pain neuroscience educator.
This is why a proper assessment needs to look at all three chronic pain mechanisms. A clinician who understands these pathways will ask different questions. They will check for widespread sensitivity. They will look at how your nervous system responds to movement, pressure, and even thoughts about movement. They will not just examine the spot that hurts.
The Role of Neuroplasticity in Chronic Pain Mechanisms
Neuroplasticity is the brain’s ability to reorganize itself. It is usually discussed as a good thing, and it often is. But neuroplasticity has a dark side. When pain becomes chronic, neuroplastic changes lock in the pain pathways. The brain literally rewires itself to be better at producing pain.
The areas of the brain that process sensation, emotion, and movement all shift their connections. The sensory cortex expands its representation of the painful body part. The prefrontal cortex, which helps with rational evaluation of threats, becomes less active. The amygdala and insula, which process emotional salience, become hyperactive. This is why chronic pain feels so emotionally heavy. It is not just a sensation. It is a whole brain state.
The hopeful part is that neuroplasticity works both ways. If the brain can learn to amplify pain, it can also learn to quiet it. This is the basis for pain reprocessing therapy, graded motor imagery, and other brain based treatments. These approaches specifically target the central sensitization and impaired descending modulation mechanisms.
Practical Steps to Address Each Mechanism
You do not need to handle this alone. But understanding which mechanism is at play helps you ask better questions when you seek care. Here is a numbered list of evidence informed steps you can take.
- Get a thorough pain mechanism assessment. Look for a physical therapist or pain specialist who uses tools like pressure pain thresholds, the Central Sensitization Inventory, and quantitative sensory testing. They can help determine which mechanisms are dominant.
- Target peripheral sensitization first if it is active. Topical lidocaine, NSAIDs, ice, and manual therapy can help desensitize local nerve endings. But do not stay here too long if symptoms persist.
- Address central sensitization with education and graded exposure. Learn how pain works. Then slowly, safely introduce movement and activity in a way that does not trigger a threat response. Pain neuroscience education alone has been shown to reduce pain catastrophizing and improve outcomes.
- Restore descending modulation through aerobic exercise and sleep. Even 15 minutes of walking or cycling can increase endogenous opioid release. Consistent sleep hygiene helps your brainstem reset its pain inhibition pathways.
- Consider medications that target the correct mechanism. SNRIs like duloxetine, gabapentinoids, and tricyclic antidepressants work on central mechanisms. Opioids and typical NSAIDs often do not. Talk to your doctor about mechanism based prescribing.
If you want to dig deeper into one of these approaches, check out this guide on building your multimodal pain management plan for a structured way to combine treatments.
Why Your Pain History Matters More Than Your MRI
One of the most frustrating experiences for people with chronic pain is being told that their MRI looks fine. That can feel invalidating. But here is the thing. MRIs show tissue structure. They do not show nervous system function. You can have a completely clean MRI and still have debilitating pain driven by central sensitization.
Conversely, you can have a bulging disc or mild arthritis and feel no pain at all. That is because pain depends on how your nervous system interprets the signal, not just the state of your tissues.
This is why understanding chronic pain mechanisms is so empowering. It shifts the focus from looking for a structural problem to understanding a functional one. You stop asking “What is wrong with my body?” and start asking “What is wrong with my pain system?” That question leads to better answers.
For a deeper look at how your brain creates and amplifies pain, read about 5 surprising ways your brain creates and amplifies pain sensations. It will change how you think about your symptoms.
Putting This Knowledge to Work
You now know the three chronic pain mechanisms that turn normal sensations into persistent pain. Peripheral sensitization makes the local alarm too sensitive. Central sensitization turns up the volume in the spinal cord and brain. Impaired descending modulation takes the brakes off the pain system.
Each mechanism needs a different approach. There is no single pill or stretch or surgery that fixes all three. But when you identify which mechanism is driving your pain, you can target your efforts where they will actually make a difference.
Start with one small step. Notice which of the three patterns sounds most like your experience. Write it down. Bring it to your next appointment. Ask your provider directly, “Do you think peripheral sensitization or central sensitization is the bigger issue for me?” That question alone can change the direction of your care.
Chronic pain is complex, but it is not random. Your symptoms follow a logic. Learning that logic is the first step toward getting unstuck. For more on the science behind your symptoms, explore this article on why pain becomes chronic and your nervous system’s role. The answers are real, and they are within reach.




